Labour & Delivery
This is the state of labour that can take days as the cervix slowly shortens and dilates. When this process needs to be hastened, prostaglandin tablets are inserted vaginally.
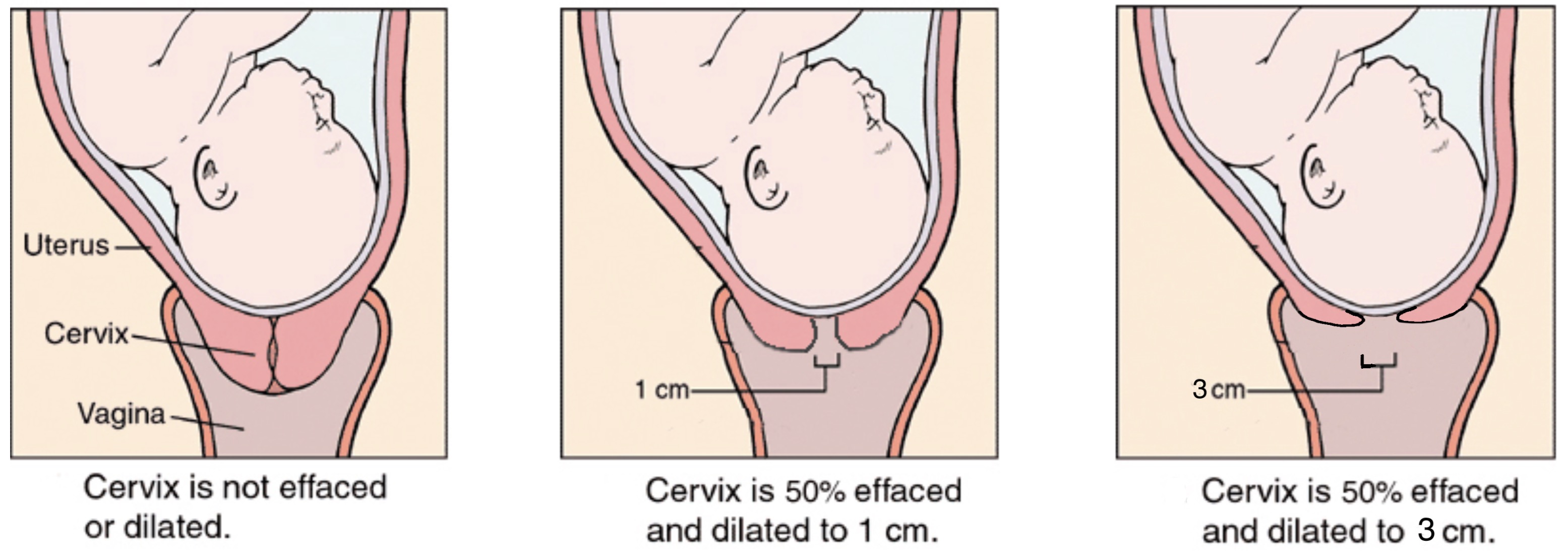
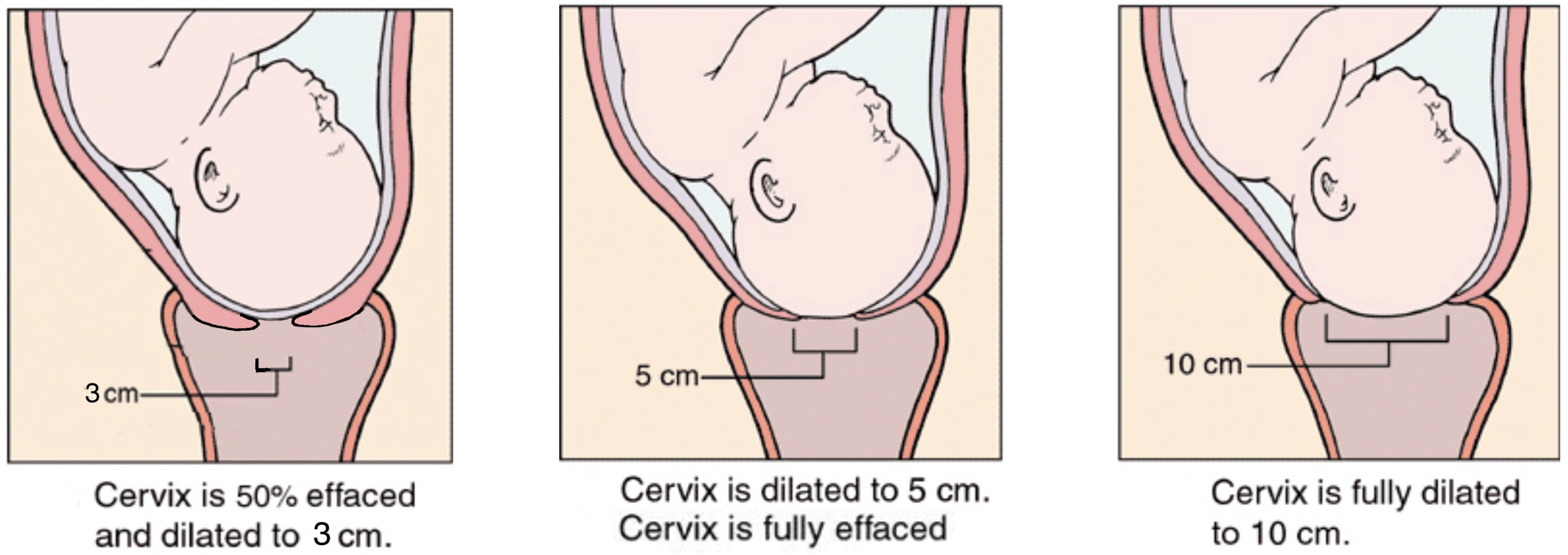
Active Phase of Labour
This is the actual state of labour where the cervix starts to become thinner, softer and dilates. The cervix can dilate at 1cm/hr till 6cm, after which it can dilate faster to reach 10cm. This phase of labour can take 6-12 hours with women in their first pregnancy taking longer.
You can make your way to the hospital when:-
- your waterbag breaks
- there is pain every 10 minutes in the last hour
- there is markedly reduced baby movement
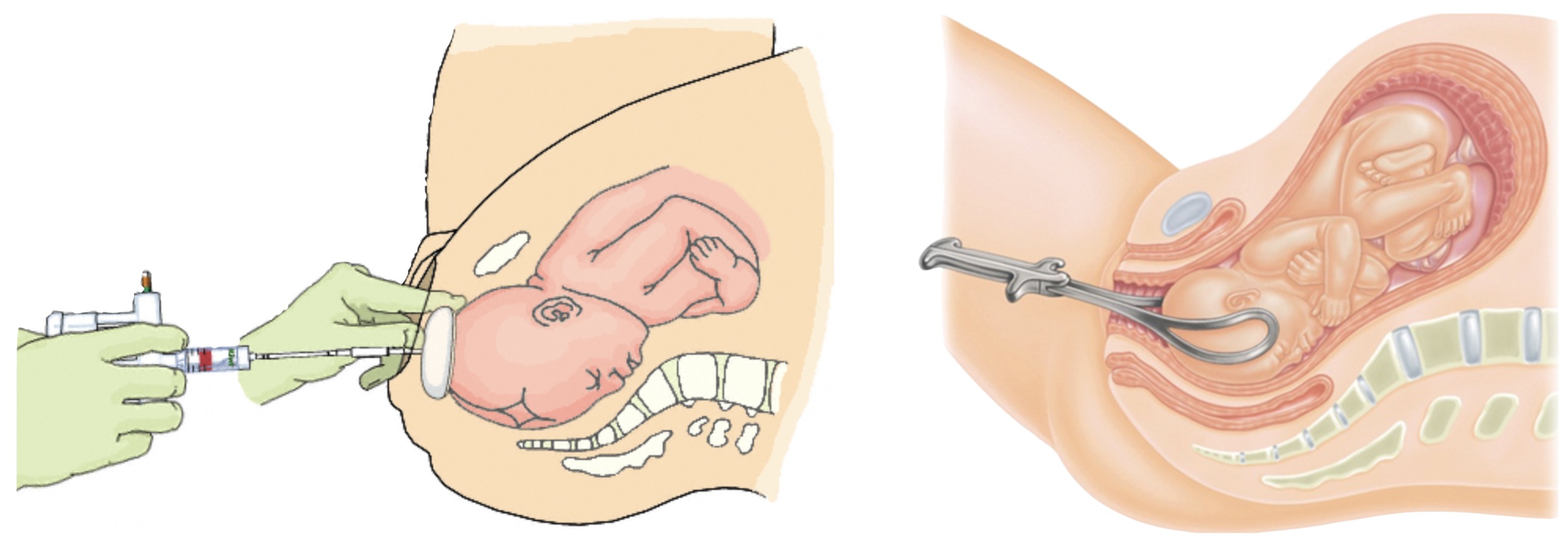
Kiwi-Vacuum Delivery and Forceps Delivery
There are risks with instrumental assisted vaginal delivery. They include
- Baby Injuries : laceration, bleeding, nerve injury, fracture
- Mother Injuries : laceration, bleeding, bladder dysfunction, episiotomy extension, bowel dysfunction, potential future incontinence and genital prolapse.
Emergency Caesarian Section
For every 10 women attempting vaginal delivery, 1 to 2 will need an emergency caesarian section.
The common reasons are:-
- Poor progress if labour where labour seems endless
- Non-reassuring fetal status or heart beat
- Cephalo-pelvic disproportion
- Profuse bleeding or severe constant pain
Non-Medical Pain Relief in Labour
- Being in good physical and mental condition to withstand the stress of labour
- Having the knowledge and a reasonable expectation of labour process
- Having a close and supportive partner during labour
- Breathing techniques, Massage and Music
- Transcutaneous Electrical Nerve Stimulation (TENS)
Medical Pain Relief
- Laughing Gas or Nitrous Oxide
- Pethidine Injections
- Epidural
Potential Problems of Labour (<1% risk)
- Bleeding
- Tears in the vaginal or anus
- Scarring and Pain of episiotomy
- Infection of episiotomy, womb or caesarian section
- Bladder dysfunction, Bowel dysfunction, Anal Fistula
- Retained Placenta or Products of Conception
Shoulder Dystocia (<0.5% risk)
- Shoulder dystocia cannot be predicted or prevented because accurate method for doing so do not exist.
- Only 1 in 4 cases of shoulder dystocia have 1 risk factor. Hence caesarian section for all at risk pregnancies to prevent shoulder dystocia is inappropriate.
- Mild shoulder dystocia may not lead to any complications.
- Severe shoulder dystocia can cause complications like bruises, fractures, nerve injuries, paralysis and brain damage.